What is an Electronic Medical Record / EMR?
An Electronic Medical Record (EMR), also called Electronic Health Record (EHR), is software that permits patient medical data to be digitally created, transmitted, and stored, as an alternative to paper medical records.
This technology is surprisingly recent and has been essential in modernizing the US healthcare system. Today there are well over 200 EMR software solutions, each with their own features that allow them some market share to compete with others. The fact that this many EMR systems persist in the same market underlines how there is no one-size-fits all solution for practitioners.

Depiction of practitioner-facing Epic EMR software.
What All EMR Systems Do:
have unique patient identifiers (deduplicating patients)
store data in an electronically (data in a medical record)
have a user interface for viewing and editing
have security features to maintain patient privacy
exporting, printing and/or faxing of data
What EMR Systems Sometimes Do:
healthcare interoperability with other systems (devices, calendars, other EMR systems, payers)
offer a patient portal for patient interactions
permit discussion between providers
billing information exchange
manage text reminders and patient communications
data analytics / population health
ordering and prescribing
medical device integration
human resources and staff scheduling / office administration
contain integrated telehealth capabilities
EMR vs EHR vs LPR
While some will debate that an EHR is the sum of all patients medical records, whereas an EMR is one hospitals instance of a patients medical records - the terms are widely interchangeable. Cerner refers to itself as and “EHR“ and Epic refers to itself as an “EMR” within their own public facing documentation. Given that these are the two largest systems, the debate is somewhat moot. In this article, we will use EMR.
Longitudinal Patient Records (LPR) are often in their own category, and refer to the aggregated information on the entirety of a patient. For large aggregators of healthcare data, creating an LPR is essential as they likely have multiple files on a single patient that should be stored in the same place. This requires creating a singular patient identity.
Categories of EMR Systems
General EMR: These are general EMR systems such as Epic, Cerner, Allscripts, AthenaHealth, and eClinicalWorks. Commonly found in major hospitals, they focus on trying to do everything. They often also engage with the payers, the government, and pharmaceutical networks. These EMRs come at a higher price and require significant resources and time for development and a safe implementation.

A rough distribution of market share
Specialty EMR: Smaller EMR systems that offer tailored services for smaller practices focusing on one specialty (dentistry EMRs, eye care EMRs, home health EMRs, etc.). These EMR systems may have unique user interfaces - for example your dentist may use a dental EMR to allow for notes on individual teeth visually with easy work flows. These are not possible with general care EMR software. Specialized EMR software often is more cost-effective as well, and easier to implement.
Here are some examples:
McKesson has an oncology EMR
Eaglesoft is a dentistry EMR
Tsystem is an urgent care EMR
Chirotouch is a chiropractic EMR
Core EHR is a mental health EMR
Lab EMR: Lab EMR system such as Quest Diagnostics focus on high healthcare interoperability to exchange data between the lab and hospitals, and offer very unique features relative to standard or specialty EMRs.
Patient Intake Tools: Many interfaces exist for supplying data to EMR systems, though they may not be an EMR themselves. One example of this is Lobbie Inc., a company that delivers HIPAA-compliant intake forms to patients and integrates directly with an EMR for data supplementation.
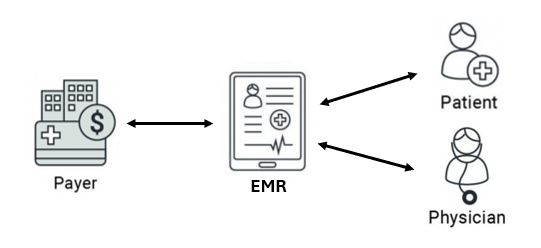
EMR Workflow
There is no one-size fits all for how patients and practitioners interact with an EMR, however it is roughly the following:
Appointment creation: A prospective patient signs up for an appointment through a patient portal in the EMR, or calls a front desk that perform this action on behalf of the patient.
Appointment communication: An EMR will commonly communicate with a patient to make sure they do no miss their appointments, and make sure they complete pre-appointment paperwork.
Practitioner Interactions: Prior to an appointment, the practitioner will review the patients available data in the EMR. During an appointment the practitioner will make notes directly on the EMR. After the appointment they will usually give the patient a print-out the visit summary to the patient, and submit any prescriptions or procedures through the EMR.
Other Facilities: Other facilities that are integrated will receive data from an EMR. This includes billing agencies, referrals to other practitioners, payers, pharmacies, or lab facilities who will then be able to act on that information.
Bill Payment: If required the patient can pay bills after services through the EMR portal.
EMR Interoperability & Storage
There is no single way that EMR data is stored - it is up to the developer of the EMR. It may use a flat database, a NOSQL database, an OODB, or even sometimes just stored as data files that are referenced when needed in a data bucket. The below diagram shows methods of how interoperability typically happens between facilities.

Most EMRs instead offer methods of exporting data for transmission, and similarly can import data from different filetypes as shown in the above depiction. See our blogs on interoperability and medical record conversion for more details. Methods of export include:
PDF/TIFF import/export many EMR systems can import unstructured PDF data, but they cant do much more with it other than display it to a user as a PDF. Similarly, they can usually export their data to a PDF
HL7 ADT messaging is a feature of largescale EMR systems that are associated with hospital systems and large medical facilities that manage inpatient and outpatient settings.
HL7 C-CDA import/export most general EMR systems can create C-CDA files as patient history snapshots, that are saved as .xml, .json, or .zip files. See our blog on C-CDA to better understand these structures. These files are relatively immobile as they are not usually associated with native API transfer. Some EMRs permit the import of C-CDA data, though it is rare.
HL7 FHIR import/export Today, nearly all modern EMR systems are capable of consuming HL7 FHIR data via API, and even more are capable of creating HL7 FHIR data.
EMR to EMR Integration is somewhat rare because most EMR systems do not want to devalue themselves by permitting 100% integration with a competing platform. However this is becoming easier as interoperability improves, as such competition is at odds with a patients quality of care. Federal policy is also mitigating this behavior more at present.

EMR Data Structure
Simply because a medical record is electronic, does not mean that is entirely structured fields that are well standardized. Both before and after export. Generally a record may broken up by the following data structures:
30% Attached files: these can be PDFs, images, videos, or just any bundled data to get thrown in with structured fields.
70% Digital Content: this is content that makes up the digital record with keys and values of medical data. This 70% may be broken down into:
60% unstructured digital data: data that, while digital does not meet a standard in how it is recorded, such as a patient note
40% structured digital data: this is data that very field-specific, codified and parse-able with tight definitions.

EMR Pros & Cons
Cons:
EMRs may cause provider abrasion (frustration) due to their technical nature and sometimes poor user interfaces
Digital records may be debatably less secure than paper records in that they can be quickly copied by a bad actor seeking to exploit medical information in cases of poor security.
Data duplication may be common in EMR systems because of poor backend development and lack of these systems wanting to permit editing of past data (but rather a copy of the new data). This can sometimes result in PDF exports of medical records to be tens of thousands of pages long in some instances.
Pros:
EMR data is faster to parse for someone looking for information in short period of time
Digital health records have better persistence as they are much easier to backup to prevent loss in a catastrophic disaster.
Data exchange speed is much faster and offers the chance to save lives the right conditions.
They are also much easier to organize.
For these reasons the US government has strong incentives to make sure that practices are utilizing electronic over paper record systems today.
Conclusion
Understanding Electronic Medical Records (EMRs) is critical to navigating the modern healthcare landscape. EMRs revolutionize patient care by offering secure, efficient, and organized data management systems, replacing the limitations of traditional paper records. While there are diverse EMR categories—ranging from general to specialty, lab-focused, and patient intake tools—they all aim to streamline medical processes and improve interoperability.
Despite challenges like high implementation costs and technical complexity, the advantages of EMRs, including data backup, faster communication, and enhanced accessibility, outweigh the drawbacks. As technology evolves, EMRs will remain pivotal in shaping a more efficient and patient-centric healthcare system.
If you would like to learn more about EMR technology and how to interact with these systems, reach out to our sales team.